
Best Price: The Benchmark That Shapes Medicaid Rebates
In the structure of U.S. drug pricing, few concepts carry as much downstream impact as Best Price. While the definition is relatively simple, the operational consequences are not. Best Price connects commercial and Medicare contracting decisions directly to Medicaid rebate liability, often in ways that are only fully understood after a contract is in motion. This dynamic makes Best Price more than a regulatory requirement. It becomes a practical constraint that shapes how manufacturers, pharmacy benefit managers, and plan sponsors approach pricing, rebates, and formulary strategy. A working understanding of how it is built and how it behaves is essential for interpreting negotiation limits and contract design choices across the market.
3/16/20265 min read

In this Episode:
The Basics
How it Works
Parallel Concepts
In Practice
Commercial and
Medicare Impacts
The Fine Print
Value-Based Contracts
Re-characterizing Rebates
Bundled Rebates
The Basics of Best Price
Best Price is a statutory concept within the Medicaid Drug Rebate Program. At its core, it represents the lowest net price a manufacturer makes available to any eligible customer in the U.S. market, with certain exclusions defined by regulation. That lowest net price establishes a benchmark that directly influences Medicaid rebate obligations.
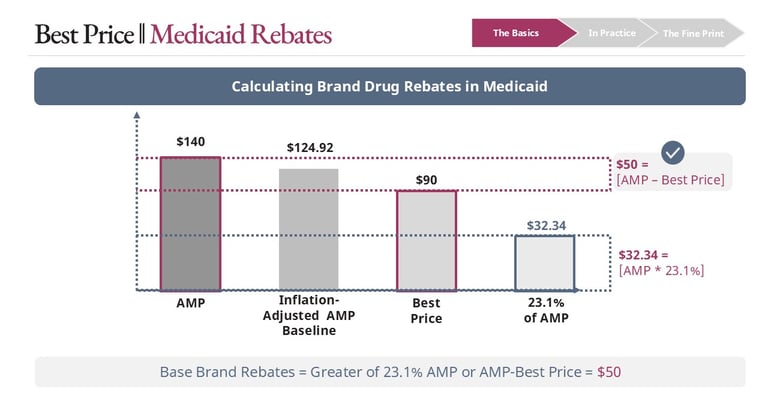
The key point is that Best Price is not tied to a single transaction. It reflects the aggregation of all qualifying concessions across customers, contracts, and channels. The lowest resulting net price becomes “Best Price.” That figure then feeds directly into Medicaid rebate calculations, where manufacturers owe the greater of 23.1% of Average Manufacturer Price or Average Manufacturer Price minus Best Price, with an additional inflation-based adjustment layered on top.
In Practice
The Fine Print
Value-based arrangements
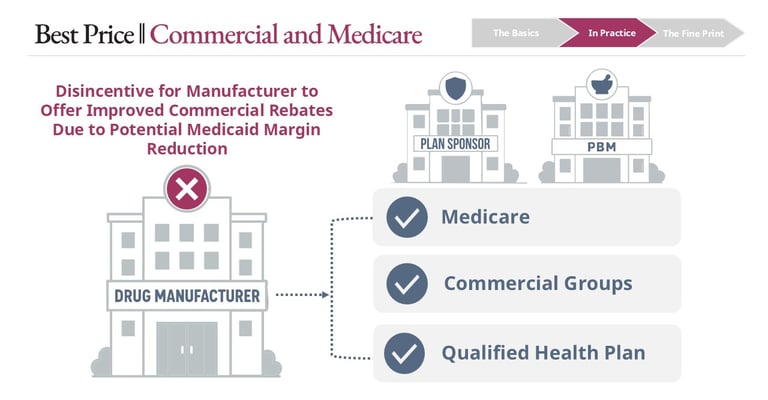
Because Best Price is derived from commercial and Medicare activity, it plays a direct role in real-world negotiations. When a pharmacy benefit manager or plan sponsor pushes for deeper rebates, the manufacturer must evaluate not just the immediate economics of that agreement, but whether the concession will establish a new Best Price. A single contract with a single counterparty can trigger increased Medicaid rebate liability across all claims for that product.
Manufacturers will often signal that additional concessions are not feasible due to Best Price exposure. While this can be interpreted as a negotiation position, it is frequently a legitimate constraint. Moving Best Price even modestly can materially increase total rebate liability, particularly for products with significant Medicaid utilization.
The mechanics of Best Price become significantly more complex when examining how different contracting structures are treated within the calculation. Not all financial concessions are evaluated equally, and subtle differences in how agreements are designed or classified can materially influence whether they impact Best Price. Understanding these nuances is essential, as small structural decisions can have broad implications for rebate liability across an entire product portfolio.
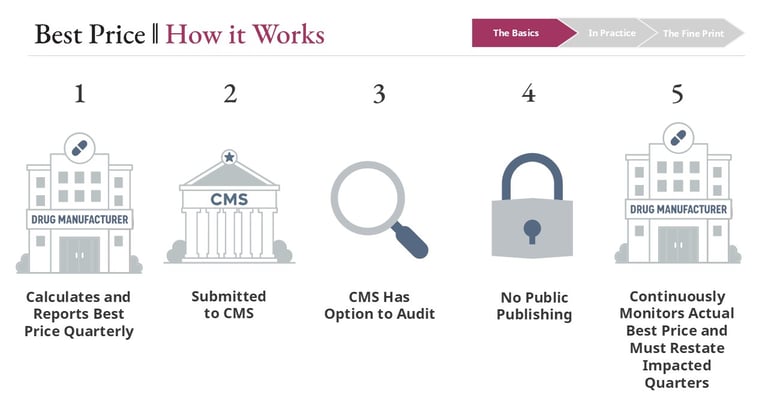
Establishment, Oversight, and Publishing
Best Price is calculated and reported by manufacturers on a quarterly basis to the Centers for Medicare & Medicaid Services. Manufacturers are responsible for maintaining accurate calculations, including revisiting prior quarters when new data or contract adjustments change the outcome. The agency has audit authority but does not publish Best Price data, in part to avoid revealing competitive pricing strategies across manufacturers.
As a result, Best Price can act as a ceiling on commercial rebate competitiveness. It introduces a tradeoff between gaining preferred formulary position in one segment of the market and preserving margin across another.
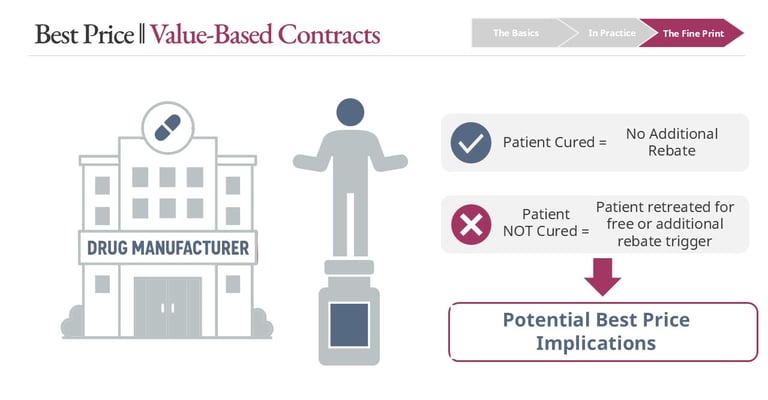
Value-based contracts add another layer of complexity. These arrangements tie payment to outcomes, such as providing additional rebates or free retreatment if a patient does not respond to therapy. While conceptually aligned with value-based care, they can create unintended Best Price implications.
If a contract results in a unit of drug being fully rebated or effectively provided at no net cost, that outcome may establish a new Best Price. Even if the scenario applies to a subset of patients, the pricing signal can extend across the entire Medicaid population for rebate purposes. Whether and how these arrangements are included depends heavily on contract structure and regulatory interpretation.
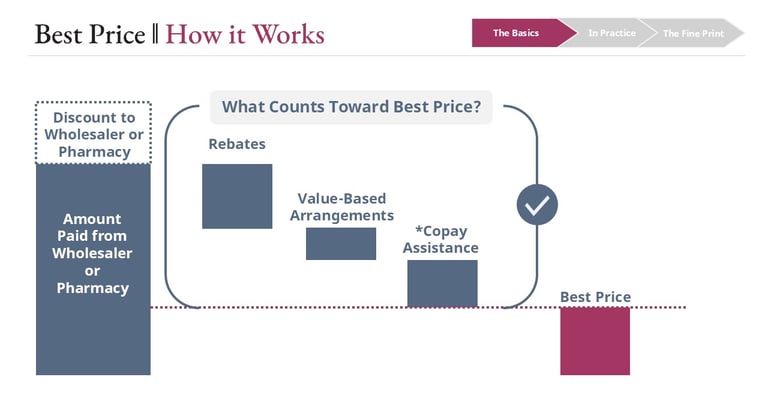
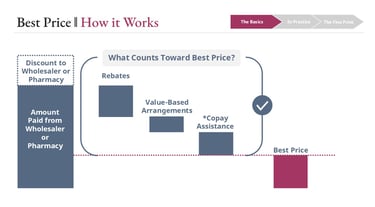
The calculation begins with the gross sales price, typically the amount paid to the manufacturer by a wholesaler or pharmacy. From there, all qualifying price concessions are considered. Rebates paid to pharmacy benefit managers or plan sponsors are the most visible component, but they are not the only ones. Price reductions tied to value-based arrangements and other financial concessions may also be considered, depending on how they are structured and classified.
This structure creates a clear incentive dynamic. Any concession that lowers the net price in one part of the market has the potential to reset the floor for Medicaid across all utilization of that drug. This is what connects localized contracting decisions to system-wide financial impact.
What’s Included in Best Price?
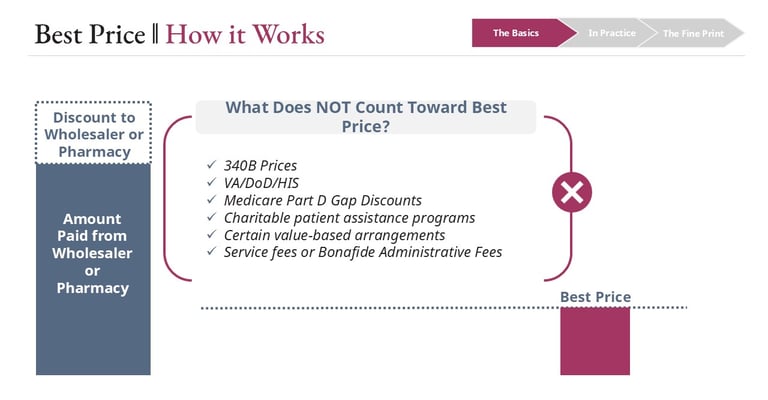
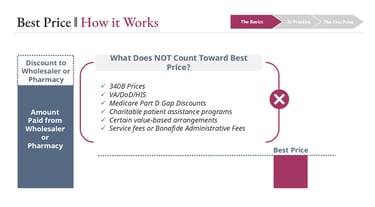
What’s Excluded from Best Price?
Not all price reductions are included in Best Price. Several categories are explicitly excluded to prevent certain programs from distorting Medicaid rebate calculations.
Prices under the 340B Drug Pricing Program are excluded, as are prices offered to federal purchasers such as the Department of Veterans Affairs, the Department of Defense, and the Indian Health Service. These programs operate under separate statutory frameworks with their own pricing rules. Discounts provided in the Medicare Part D coverage gap are also excluded from Best Price.
These exclusions function as guardrails. Without them, already-discounted programs could unintentionally drive higher Medicaid rebate obligations.
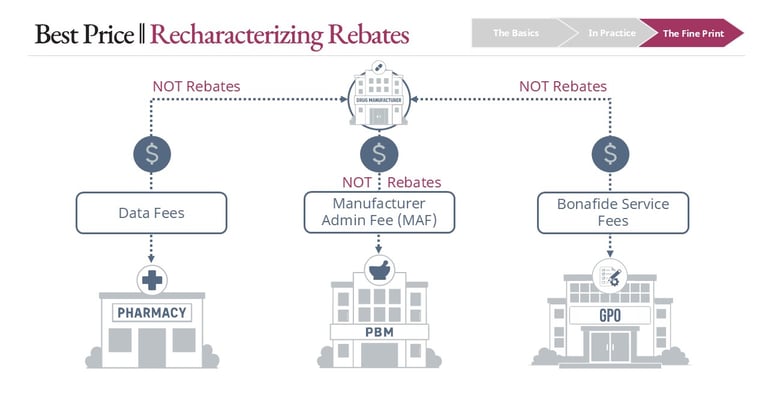
Service fees and classification
The distinction between rebates and service fees is another critical detail. Manufacturers often pay fees to pharmacy benefit managers, specialty pharmacies, or group purchasing organizations for administrative services, data access, or contract facilitation. When these payments meet the definition of bona fide service fees, they are excluded from Best Price.
However, if a fee is tied to formulary placement or utilization in a way that resembles a rebate, it may be reclassified and included. The characterization of these payments is not just semantic. It directly determines whether they affect Best Price calculations.
Conclusion
Bundled arrangements
Bundled rebate contracts introduce additional complexity. In these arrangements, manufacturers link multiple products together, offering improved economics if a plan provides favorable placement across a portfolio.
Even when the rebate change is isolated to a single product within the bundle, the structure of the agreement can cause Best Price to shift for all included products. Because the concessions are contingent on combined performance or placement, the pricing signal is treated as shared across the bundle. This can extend Best Price exposure beyond the product that initially drove the change.


Best Price is a foundational mechanism that ties together multiple segments of the drug pricing system. It translates localized contracting decisions into system-wide financial consequences, particularly within Medicaid. For manufacturers, it defines the boundary of how far pricing concessions can go without triggering broader liability. For pharmacy benefit managers and plan sponsors, it explains why certain rebate discussions plateau despite apparent competitive pressure.
Understanding Best Price requires more than knowing its definition. It requires recognizing how different types of concessions are treated, how contracts are structured, and how seemingly isolated decisions can propagate across the market. As pricing models continue to evolve, especially with increased interest in value-based and portfolio contracting, Best Price will remain a central consideration in how strategies are designed and executed.
Note: Not all Copay Assistance dollars count toward Best Price. Copay assistance dollars generally only count toward best price in circumstances where value of copay assistance accrues to the plan sponsor via accumulator adjustment programs.
Links
hello@thecoypharmer.com
© 2025 The Coy Pharmer, LLC. All Rights Reserved.